Over the past few weeks, social media posts and articles like “The Quiet Reality Behind Vaping and Smoking” on The Home Channel in South Africa have been circulating widely. These pieces tap into real concerns about health, addiction and youth use—but they also present misleading or flat-out incorrect information about vaping. This post breaks down the key claims in these articles and debunks them with what the evidence really shows, using sources such as the UK Office for Health Improvement and Disparities (OHID), the Royal College of Physicians (RCP), Cancer Research UK (CRUK), the Cochrane Collaboration, the New Zealand Ministry of Health, and others.
If we’re serious about reducing smoking-related disease, then we owe the public the full picture—not claims that sound scientific but contradict what major independent health bodies actually say.
Claim 1: “Vaping carries its own chemical load, similar to smoking.”
The evidence: The chemical profiles are not comparable. Not even close.
Cigarettes burn tobacco at over 600°C, creating smoke containing over 7,000 chemicals, around 70 known carcinogens, plus carbon monoxide and tar. This toxic cocktail is what kills up to two-thirds of long-term smokers.
Vaping, by contrast, does not involve combustion.
Typical e-liquid contains only four components:
propylene glycol (PG), vegetable glycerin (VG), flavourings, and nicotine (optional).
The UK’s 2022 OHID evidence review—conducted by King’s College London—found that vapers have dramatically lower levels of carcinogens and toxins than smokers. HERE
Cancer Research UK notes the same: biomarkers of cancer-causing chemicals drop significantly when people switch from smoking to vaping. HERE
Canada Health highlights that, “[vaping] Immediately reduce their exposure to the harmful chemicals found in cigarette smoke. HERE
Yes, vaping has a chemical load — but the type and quantity of chemicals are nowhere near those produced by burning tobacco.
Claim 2: “Vaping causes Popcorn Lung”
This myth refuses to die, despite being debunked repeatedly by medical authorities.
What is Popcorn Lung?
Bronchiolitis obliterans—nicknamed “popcorn lung”—was first found in popcorn factory workers inhaling large quantities of diacetyl used in butter flavouring.
What do health authorities say?
Cancer Research UK:
“E-cigarettes don’t cause the lung condition known as popcorn lung.
There have been no confirmed cases linked to e-cigarette use.” – HERE
UK Health Security Agency:
The agency points out that where diacetyl was found in some early e-liquids, levels were hundreds of times lower than in cigarettes. Yet cigarette smokers—who inhale far more diacetyl—do not develop popcorn lung. – HERE
In the UK and EU, diacetyl has been banned in e-liquids since 2016, making the claim even more outdated. Research conducted in 2021 and funded by the Government of Canada, Health Canada, tested 825 vape e-liquids available in their country, and found only two samples that contained diacetyl. These two samples were manufactured before 2018. – HERE
So why does the myth persist?
Because it’s frightening and memorable. But based on real-world data:
- Cigarettes contain far more diacetyl than early e-liquids ever did – HERE
- Popcorn lung has not been observed in smokers
- No confirmed cases exist in people who vape
In short: popcorn lung is not a vaping-related disease.
Claim 3: “Vape liquids contain oils and behave like cooking spray.”
This is factually incorrect.
E-liquids are not oils.
Standard nicotine e-liquids are made from PG and VG—water-soluble compounds used in asthma inhalers and food products. They are not lipids and do not behave like oils when inhaled. – HERE
So why the confusion?
Because of the 2019 U.S. EVALI outbreak
The lung injuries seen in the US were overwhelmingly linked to vitamin E acetate used in illicit THC cartridges, not nicotine vaping. – HERE
CDC findings:
- Vitamin E acetate was found in lung fluid of affected patients
- Most cases involved black-market THC cartridges
Countries with regulated nicotine products (e.g. UK, New Zealand, European Union) did not experience a similar outbreak.
So no—regulated vape liquids do not contain oils and do not behave like cooking spray.
Claim 4: “When it comes to smoking vs vaping, there’s no clear winner.”
This claim directly contradicts the findings of nearly every credible public health authority.
Royal College of Physicians (UK)
UK OHID (formerly Public Health England)
Cancer Research UK
New Zealand Ministry of Health (Vaping Facts)
The NZ government promotes vaping as a quitting tool for adults who smoke. – HERE
Cochrane Collaboration (2025 update)
The gold-standard evidence review finds:
- High-certainty evidence that vaping helps more smokers quit than nicotine patches or gum
- No serious harms detected in studies up to two years
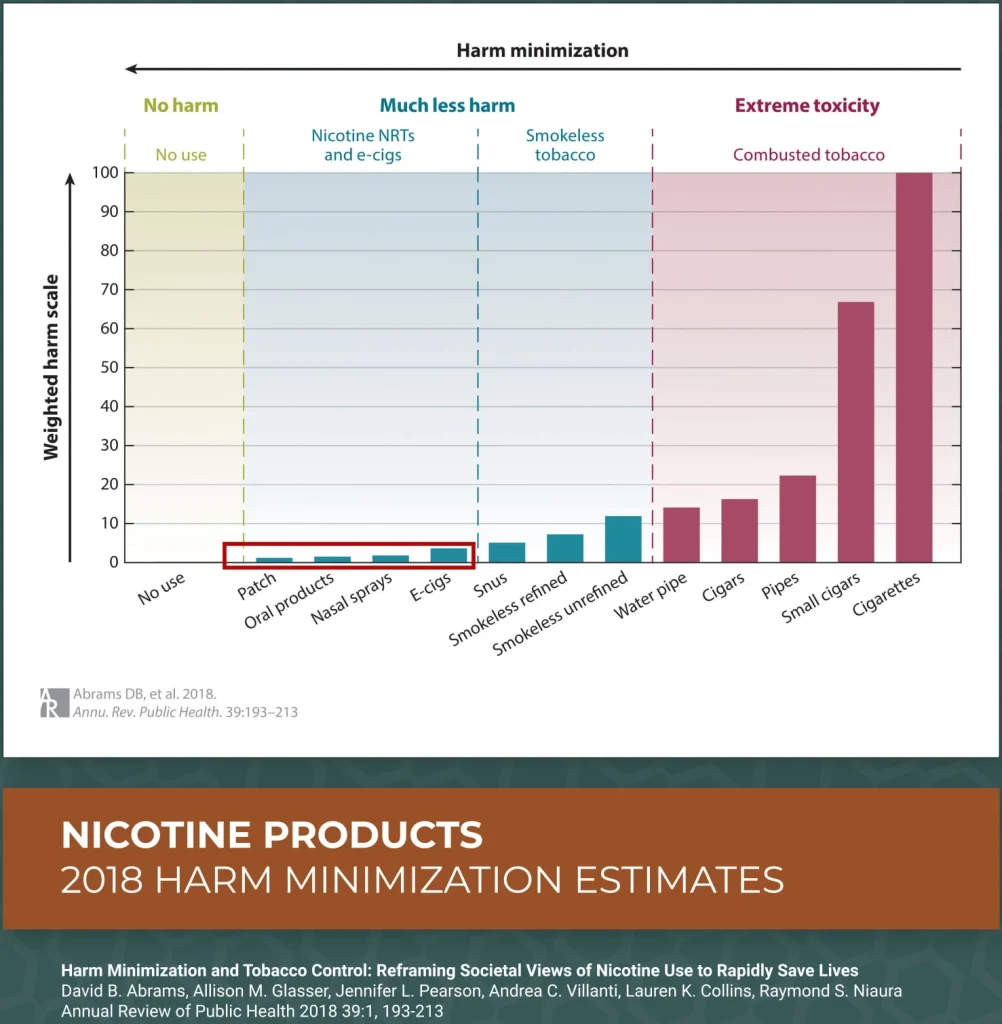
So what does the continuum of risk actually look like?
Health authorities across the world now recognise the following hierarchy:
Lowest risk → Highest risk
- No nicotine use
- Nicotine Replacement Therapy (patches, gum)
- Regulated nicotine vaping
- Heated tobacco products
- Cigarettes and all combusted tobacco
Vaping is not risk-free—but it is vastly less harmful than smoking. Pretending they are equal only keeps smokers smoking.
Why these myths are dangerous
Articles like the one circulating on social media often have good intentions—concern about youth, addiction and health. But misinformation has consequences.
When adults who smoke see claims like “vaping is as bad as smoking”, many simply continue smoking—the product that kills 50–67% of long-term users.
That is the opposite of harm reduction.
What the public deserves is clarity:
1. If you don’t smoke, don’t start vaping.
2. If you smoke, switching to a regulated vape is far less harmful than continuing to smoke.
3. If you vape to quit smoking, aim to eventually quit vaping too.
4. Youth access must be strictly controlled.
This is the balanced, evidence-based approach supported by global health authorities—not the exaggerated fears currently dominating social media.


